Event: European Conference on Rare Diseases & Orphan Products (ECRD 2026)
Place & date: O2 Universum, Prague & online, 3–4 June 2026
Organiser: EURORDIS – Rare Diseases Europe, with Orphanet
From 3 to 4 June 2026, the European Conference on Rare Diseases & Orphan Products (ECRD 2026) took place at the O2 Universum congress centre in Prague – the largest patient-led policy event on rare diseases in Europe. Attending on behalf of the Swiss Angiodysplasia Association, I took part in several programme sessions over two intense conference days – including the Poster Pitches on both days. In the following report I would like to summarise my key takeaways from the conference.
More than 30 million people in Europe live with one of over 7,000 rare diseases. Despite considerable progress, the field remains marked by fragmentation – in diagnosis, care, research and access to therapies. This is exactly where ECRD 2026 came in, held under the theme “Rare Diseases in a Changing & Competitive Europe” and closely tied to the development of a European Blueprint for Rare Diseases. Such a “blueprint” is a jointly developed framework for action that consolidates existing knowledge, policy recommendations and the perspectives of all stakeholders into a concrete basis for a future EU Action Plan.

Overview: sessions attended
- Day 1 – Holistic care: patient-centred and evidence-based (C1)
- Days 1 & 2 – Poster Pitches: research from the community
- Day 1 – Filling the gaps in evidence-based care (C2)
- Day 2 – Mental health in rare conditions (F1)
- Day 2 – Access to specialised healthcare: what should we measure? (D2)
- Day 2 – Closing plenary: the Blueprint and the way forward
The common thread: a European Blueprint
The focus was clear from the opening plenary: ECRD 2026 saw itself as a milestone on the way to a European Blueprint for Rare Diseases. This Blueprint is intended to consolidate existing knowledge, policy recommendations and the perspectives of all stakeholders into a workable framework, and to form the basis for an EU Action Plan as well as for the global WHO Action Plan. Across all six thematic tracks – from therapy development through diagnosis, holistic care, specialised healthcare and reimbursement to mental health – ran one question: how can scientific and regulatory progress be shaped so that it actually reaches people and reduces inequalities across Europe?
One aspect ran through practically every session – from the plenary to the expert talks: patient involvement. Time and again it was stressed that people affected are not merely a target group, but must be active co-creators of research, care and policy.
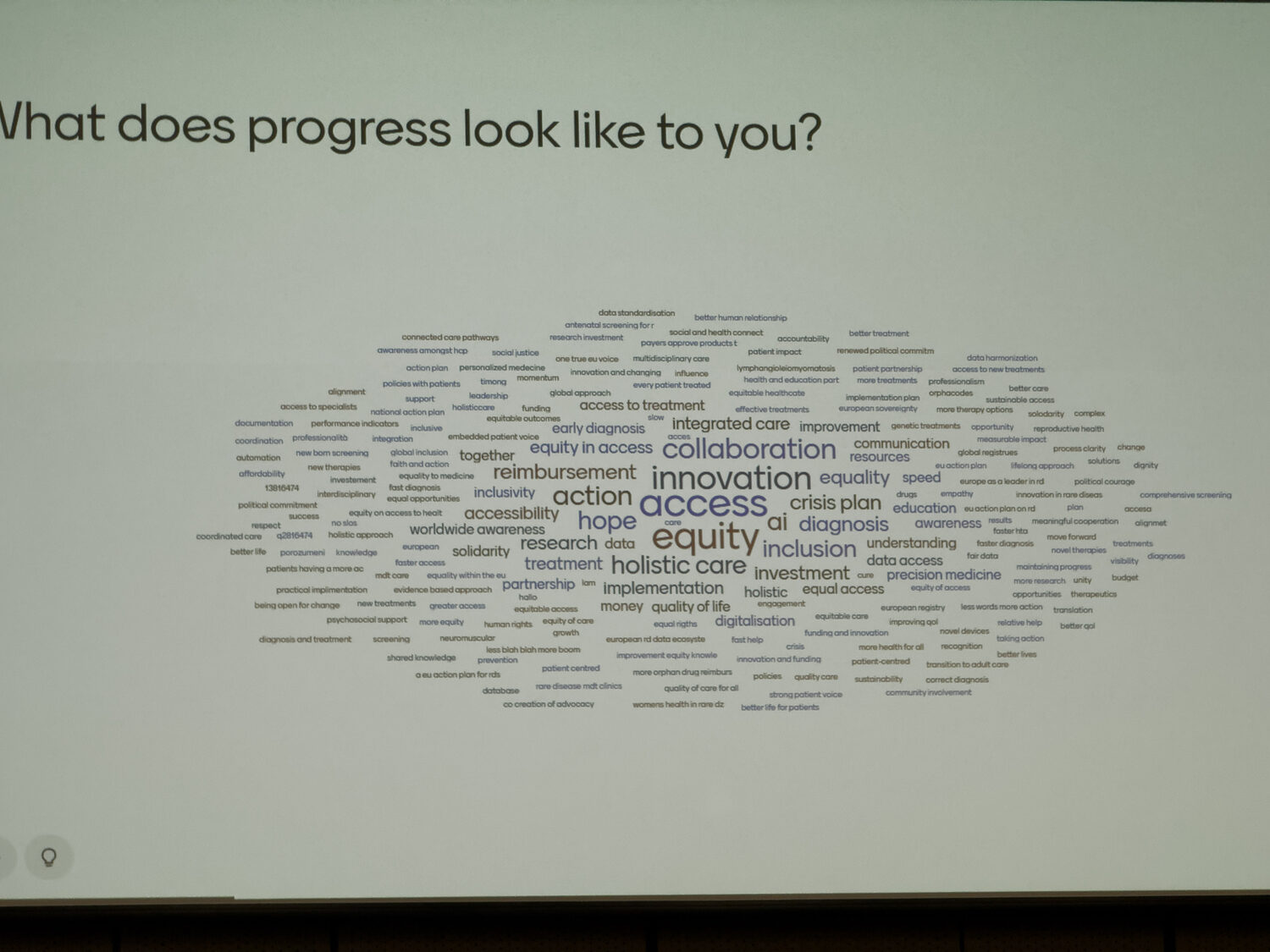
A good example of this involvement was an interactive element right at the start: all participants could enter live, via their phones, what “progress” means to them personally. From the answers of everyone present, a word cloud emerged in real time, dominated by terms such as access, collaboration, equity and innovation – a fitting summary, written by the community itself, of what drives people.

Day 1 · Wednesday, 3 June
Holistic care – patient-centred and evidence-based
Track C, Session 1 · 11:00–12:30
“Advancing Holistic Care for Rare Conditions: A Patient-Centred and Evidence-Based Approach”
Moderator: Claudia Crocione (HHT Europe) · with, among others, Jessie Dubief (EURORDIS), Iolo Eilian (HSE Ireland), Dr Roser Francisco (Hospital Sant Joan de Déu, Barcelona), Arne Noppe (Sciensano), Dr Rohita Sharma (Alexion)
This session was relevant to me for a particular reason: it was moderated by Claudia Crocione of HHT Europe – the European umbrella organisation for hereditary haemorrhagic telangiectasia, a vascular disorder closely related in subject matter to angiodysplasia. The discussion centred on what “holistic care” means in practice and how it can be underpinned by robust evidence.
The starting point was a sobering finding from EURORDIS’s Rare Barometer surveys: most people with a rare disease do not expect a cure by 2030, but believe that their quality of life could be significantly improved through better access to holistic care. Care coordination and psychosocial support have for years been among the greatest unmet needs.
Patient surveys as evidence – but done properly
One focus was the methodology of patient surveys. If patient organisations want their survey results to hold up before decision-makers, the evidence must be robust and withstand critical scrutiny. Topics included: working with representative samples rather than the entire population, using validated questions that allow comparison with the general population, and honestly communicating what the data cannot tell us. EURORDIS draws on a panel of more than 25,000 people and makes the analyses available to participating organisations for their own work.
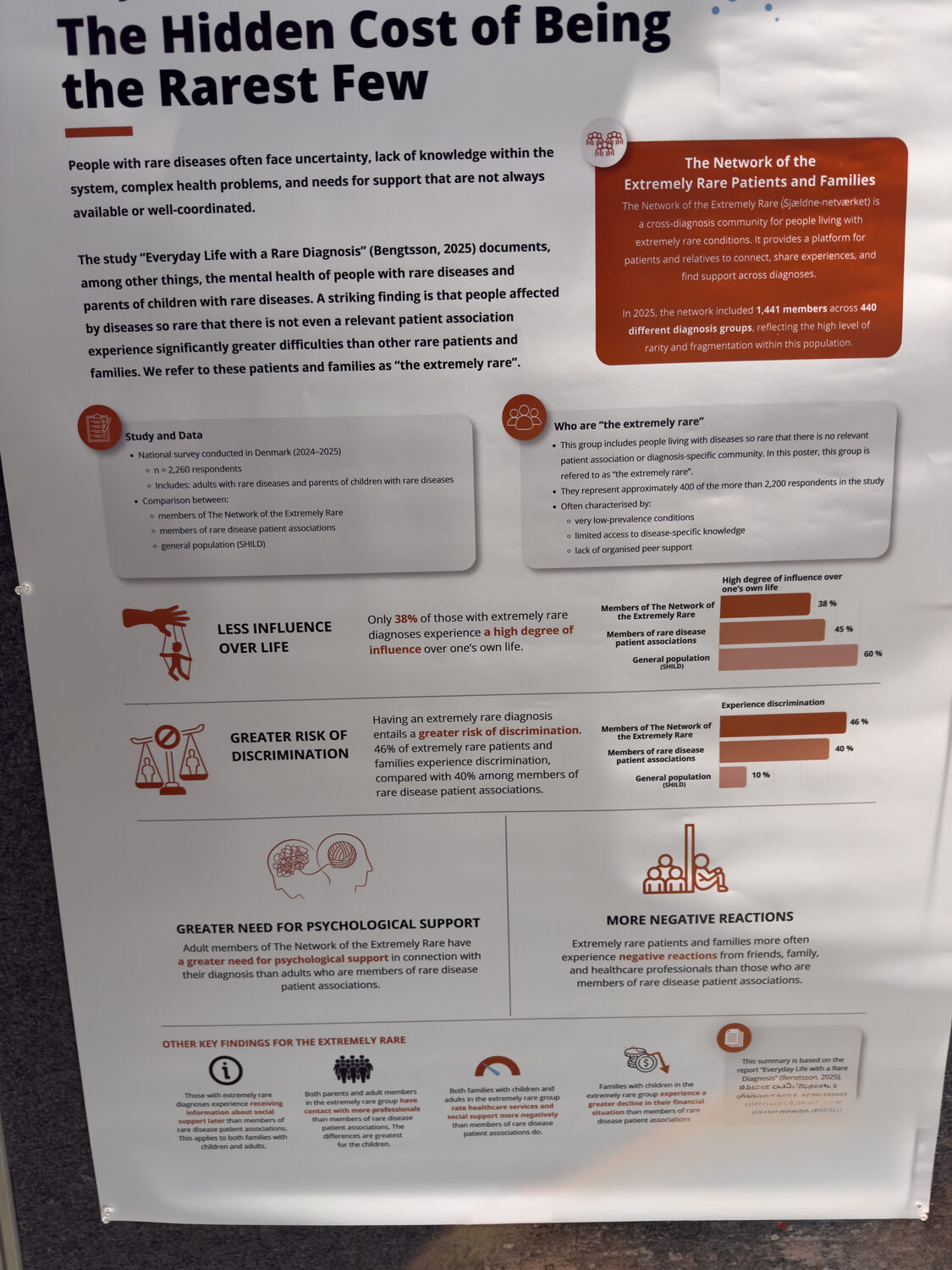
The “hidden costs” of rare diseases
Particularly striking was the presentation of a cross-country cost-of-illness study. It made visible what system-based data (for example from billing systems) precisely fail to capture: the direct non-medical costs and the out-of-pocket expenses of those affected – from paid care and long-term care to services that no healthcare system covers. The message: good data only emerges when lived experience, figures and policy come together. “We don’t want healthcare systems built on assumptions,” was the consensus – but rather systems built on the real experience of those affected.
“If we only look at system-level data, we don’t see what the patient community absorbs out of its own pocket along the way.”
This was complemented by a disease-burden estimation model (Sciensano) that mathematically combines the many symptoms of a person into a comparable measure of quality of life and years lost – a tool to give policymakers and industry comparable, robust metrics.
From measuring to co-creating: PREMs and partnership
From Barcelona, the Catalan programme for rare diseases was presented, which works with PREMs: Patient-Reported Experience Measures are standardised questionnaires through which patients themselves assess how they experienced their care – such as accessibility, coordination and communication. This systematically embeds the patient experience as an evaluation indicator – combined with instruments for person-centred care. From Ireland came an example of a consistent partnership model: six regional councils in which patients, families and professionals jointly shape care and policy – “co-design” rather than mere consultation.

Why this matters for us
Combining lived experience, sound methodology and economic arguments is exactly what a small patient organisation needs in order to be heard by authorities and payers. The proximity of HHT Europe to the topic underlines how valuable European networking is, especially for vascular disorders.
Days 1 & 2 · 3–4 June
Poster Pitches – research straight from the community
Day 1: 14:00–15:30 · Day 2: 11:00–12:30
Short presentations of the top-scoring posters, each followed by an audience vote for the ECRD 2026 Poster Awards.
The Poster Pitches were a highlight for me on both conference days: researchers and patient advocates presented their work in short, pointed pitches, making you want to take a closer look at the posters themselves. Several contributions stood out in particular:
- Clinical guidelines for connective tissue disorders: A systematic review mapped recommendations for rare connective tissue disorders (which affect several organ systems at once). The conclusion: the problem is less a lack of recommendations than their accessibility – they are fragmented across specialties, and patients effectively become coordinators of their own care. A “clinical toolkit” developed jointly with patient partners aims to address this.
- Prioritisation for therapies (ATMP): A framework scores rare diseases on dimensions such as medical need, psychosocial burden and “research readiness” (e.g. availability of registries) – partly supported by AI-assisted research – to make decisions about advanced therapies more transparent.
- Citizen-driven genomics: The moving account of a father (a lawyer) whose child has an extremely rare disease with a short life expectancy. Out of his own experience he founded a foundation and built a platform through which people affected in more than 20 countries share their genomic data – research driven by the community itself.
Day 1 · Wednesday, 3 June
Filling the gaps in evidence-based care
Track C, Session 2 · 17:00–18:30
“Filling the Gaps to Provide Evidence-Based Holistic Care”
Moderator: Jessie Dubief (EURORDIS) · with, among others, Prof. David Keegan (ERN-EYE), Dr Pauline Nauroy (Fondation Maladies Rares), Dr Solange Roumengous (APHP – BNDMR), Dr Natalie Uhlenbusch (UKE Hamburg), Eva-Maria Strömsholm (patient advocate)
The follow-up session addressed the open flank of holistic care: there is a lack of clear definitions, and many studies measure narrow clinical endpoints instead of what really matters to patients – which makes results hard to compare. The key lies in making better use of existing data.
Registries as the backbone of evidence
From France, the BNDMR was presented – the national database for rare diseases, built since 2011 as part of the second national plan. It links the local, national and European levels, is designed for interoperability and the future European Health Data Space, and entering a new patient takes only five to six minutes. Prof. David Keegan used the example of the ERN-EYE registry for rare eye diseases (ERN = European Reference Network, an EU-wide alliance of specialised centres for a disease group) to show how demanding – but worthwhile – it is to build interoperable, legally compliant registries across borders. Data protection and legal clarity (GDPR) proved just as critical as the technology.
Social sciences and psychological self-help
A further contribution argued for involving the social sciences and humanities (SSH) more strongly in care research – for instance through a dedicated funding line within the European Joint Programme on Rare Diseases. Specifically, the Q.RARE.LI project (University Medical Center Hamburg) was presented: a brief, low-threshold psychological self-management programme that was tested in a randomised controlled trial (including in Marfan syndrome and neurofibromatosis) and demonstrably and lastingly improved quality of life. It is scalable, peer-supported and usable internationally – a model for pragmatically closing the psychosocial care gap.
“I feel like I can accept this as my new normal now and have a future without fear and despair.”
— from the patient perspective on the Q.RARE.LI programme
Day 2 · Thursday, 4 June
Rethinking mental health in rare conditions
Track F · 09:00–10:30
“Rethinking Mental Health in Rare Conditions: From Undefined Challenges to Collaborative Solutions”
Chair: Dr Kirsten Johnson (Fragile X International) · with Isabella Brambilla (Dravet-Italia), Jessie Dubief (EURORDIS), Dr Stewart Rust (Manchester University NHSFT), Vinciane Quoidbach (European Brain Council), Dr Jane Waite (Cerebra Network)
This was one of the most striking sessions for me. For many rare diseases, mental health is not just a side effect but a core feature – biologically, psychologically and socially driven. Isabella Brambilla (Dravet-Italia) described the image of an iceberg: the symptom is visible, while beneath it lie autonomy, cognitive abilities, social relationships and the burden on the whole family. Her key sentence: “If we focus only on the symptom, we lose sight of the person.” Acceptance – by the person affected and within the family – is the first, often missing foundation of any successful care.
Data that shake you up
EURORDIS presented, for the first time, results of a Rare Barometer survey on mental health (around 10,000 participants, GDPR-compliant, using validated scales). Depression, anxiety and above all loneliness occur many times more frequently among people with rare diseases than in the general population. A central unmet need: access to reimbursed psychological support. Many of those affected reported being left alone during the diagnostic process and sometimes needing a whole year to accept the diagnosis – those who received support coped noticeably better.
The family at the centre
The paediatric psychologist Dr Stewart Rust (Manchester) highlighted the enormous burden on relatives: the “diagnostic odyssey”, the feeling of being misunderstood, the pressure to become an expert oneself, and even a measurably higher risk of relationship breakdown. Programmes such as the “Tree of Life” approach give children and young people a safe space to talk about their condition and build resilience. Vinciane Quoidbach (European Brain Council) added the perspective of “brain health” across the entire lifespan – with particular attention to the often precarious transition from paediatric to adult care.
In an open round that followed, the audience gathered suggestions for what mental health provisions should go into the EU Blueprint: a consistently biopsychosocial approach, research funding on “brain health”, free psychosocial and rehabilitative services (modelled on the Austrian example) – explicitly for adults too – psychologists firmly integrated into care teams, and targeted support for family resilience.
Day 2 · Thursday, 4 June
Access to specialised healthcare – what should we measure?
Track D, Session 2 · 14:00–15:30
“Rethinking Access to Specialised Healthcare for PLWRD – What Should We Measure?”
Chairs: Dr Enrique Terol (Permanent Representation of Spain to the EU) & Ines Hernando (EURORDIS) · Keynote: Dr Marina Karanikolos (European Observatory on Health Systems and Policies) · with Charline Maertens (KCE Belgium), Natalie Frankish (Genetic Alliance UK), Dr Anne-Sophie Lapointe (France)
As central as access to specialised healthcare is, it is – as this session showed – hardly measured in a consistent way. Often there is only a single metric per country; Spain, for example, surveys patient satisfaction. This makes international comparisons difficult.
A framework for measurement
Dr Marina Karanikolos presented the Health System Performance Assessment framework and translated it to rare diseases. Access can be captured along several dimensions – whether services are approachable, available, affordable and appropriate – embedded in quality, equity, financing, governance and the availability of a workforce. The appeal: consistently include rare diseases in the performance assessment of health systems in order to make systemic drivers visible.
From need to metric
Another instrument captured unmet needs through patient questionnaires. One figure stuck: a considerable share of those affected wait more than two years for their first contact with a specialised service. The panel discussion focused on which few, meaningful indicators belong in a policy dashboard: time to diagnosis, transition rates from paediatric to adult medicine, PREMs and quality of life. The role of primary care as the actual entry point into the system was emphasised repeatedly – along with the difficulty, in federal systems (e.g. the four nations of the UK), of establishing a common baseline at all.

Day 2 · Thursday, 4 June
Closing plenary – the Blueprint and the way forward
16:00–17:15 · Conference Wrap-up & Closing Plenary
with, among others, Vicky McGrath (Rare Diseases Ireland), Dr Enrique Terol, Dr Holm Graessner (HLM4RARE) · panel with Members of the European Parliament · messages from DG Santé, WHO Europe, EESC and EUCOPE · closing: Avril Daly & Jean Saslawsky (EURORDIS)
The closing plenary distilled the two days into a political message. At its centre, once again, was the European Blueprint as the “architecture” for sustainable policy: the tools and the knowledge already exist – they are simply not reaching people fast enough. Several Members of the European Parliament pledged to push for a binding EU Action Plan and corresponding Council conclusions.
One forward-looking theme: the European Reference Networks (ERNs) are to evolve from care networks into innovation networks that themselves generate evidence, diagnostics and treatment. Added to this were impulses on the European Health Data Space, on cross-border care, and on the new HTA Regulation, which from 2025 shapes the joint clinical assessment of medicines. A video message from WHO Europe (Dr Natasha Azzopardi-Muscat) anchored it all globally: no one should be left behind – including people living with a rare disease.

Conclusion for the Swiss Angiodysplasia Association
Two days of ECRD 2026 showed that the big questions of rare diseases – diagnosis, holistic and specialised care, mental health, reimbursement – are similar across all disease areas. From a Swiss perspective in particular, one thing becomes especially clear: because the number of people affected per disease is small, we depend on cooperation with our neighbouring countries – in research, care and political advocacy. For a small association like the Swiss Angiodysplasia Association, my main takeaways are:
- Cross-border cooperation is decisive: For a small country like Switzerland – with correspondingly few people affected per disease – exchange with neighbouring countries and through European structures such as HHT Europe and the European Reference Networks (ERNs) is the key to pooling enough knowledge, case numbers and resources.
- Evidence beats anecdote: Well-designed patient surveys and cost-of-illness data are the strongest argument vis-à-vis authorities and payers.
- The patient experience counts: Patient-Reported Experience Measures (PREMs) make measurable how those affected actually experience their care – an instrument we should demand and use more.
- Mental health is not an add-on: It must be a self-evident component of all care – for those affected as much as for their families.
- Shape it, don’t watch it: With the Blueprint and a future EU Action Plan, the political framework for rare diseases is taking shape right now. For Switzerland it is important to help shape this development actively through cooperation, rather than merely following it.
About this report. Written on the basis of the official ECRD 2026 programme, the author’s own photos and audio recordings of the sessions attended. Names and roles follow the official programme; individual figures from the talks have been rendered in substance.